Intelligent Technologies for Self-Sustaining, RFID-Based, Rural E-Health Systems
By Stanley Chia, Ali Zalzala, Laura Zalzala, & Ali Karimi
NOTE: This is an overview of the entire article, which appeared in the Spring 2013 issue of the IEEE Technology and Society MAGAZINE.
Click here to read the entire article.
The authors point out the importance of community-based healthcare in emerging economies. But access to patient medical records can be a problem in this setting, as paper records can be stored at a central facility that is remote from the point of care. This could lead to errors in diagnosis, medication and treatment. They propose a radio frequency identification (RFID)-based community e-health system where a patient is given a “passive” RFID card or an equivalent device (such as a stylized bracelet) and the community healthcare workers are each given a mobile RFID read/write device that can also access the central electronic medical record system. to be complex. They have studied how to implement this model in such a way that it is self-sustaining, rather than relying on recurring external funding, such as charitable support.
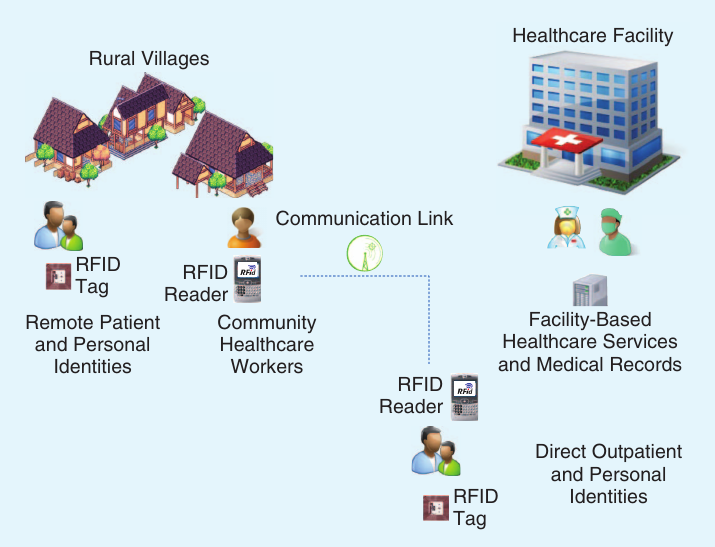
The authors point out that the concept of the use of RFID devices for public health in developing countries is not new, but that their proposal leverages collaboration between community healthcare workers and a central medical facility to design a sustainable solution that can potentially improve the quality of life for people at remote, rural locations.They discuss the RFID device and the system configuration in which they could be used.
The operation of the system will require a patient to bring his/her RFID medical card when visiting a community healthcare worker or the central facility. When a patient interacts with a healthcare worker in the field or at the central medical facility, the patient’s RFID medical card will be read to verify the person’s identity. This will also facilitate the download of the most up-to-date version of the person’s medical record information from the central database to the mobile RFID device. At the conclusion of the healthcare service transaction, the healthcare worker can update both the RFID medical card as well as the central medical record database. They point out that this scenario assumes that mobile communication coverage is available at the point of care. If it is not, the central database will have to take place offline.
The authors suggest several possible business models, such as fee splitting and micro-health-insurance plans. The aim is to be able to cover capital and recurring costs plus perhaps a reasonable profit. The article includes a quantified example of such a healthcare system, in a self-sustaining situation.
ABOUT THE AUTHORS
Stanley Chia (Stanley.Chia@vodafone.com) is with Vodafone Group R&D, U.S.A.
Ali Zalzala (zalzala@communitytracks.com) is with Community Tracks, U.S.A.
Laura Zalzala (laura.zalzala@aue.ae) is with American University in the Emirates, UAE.
Ali Karimi (ali.karimi@ieee.org) is with Trans Technology Group, U.S.A.
