A Real-time Collaborative Tele-ultrasonography System Applied to Underserved Communities
A Real-time Collaborative Tele-ultrasonography System Applied to Underserved Communities
By Alécio Pedro Delazari Binotto
NOTE: This is an overview of the paper which describes the project.
Click here to read the entire paper.
This paper presents the results of a real-time tele-ultrasonography system applied to communities far from high-complexity hospitals. Statistics from the Brazilian public health service show a miss rate higher than 30% in obstetric ultrasonography exams in Porto Alegre city, and more than 60% in the Restinga community. Additionally, the time gap of at least 4 months between the local exam request, by the periphery health center physician, and its realization in the main hospital was unacceptable. The PoaS@ude project presents a low-cost tele-ultrasonography system applied at Restinga neighborhood, where examinations are carried on the outskirts’ health center accompanied in real-time by a specialist physician located on the reference hospital at the central city of Porto Alegre. During the project, the examination miss rate decreased to less than 10% and the exam waiting time to less than 30 days. Finally, the results obtained during the pilot made the project to evolve towards a permanent service, being the solution easily reproduced elsewhere.
The PoaS@ude project, presented in this paper, is a telemedicine initiative where the exam report responsibility belongs to the remote specialist doctor located at the referral hospital, i.e., it is the first medical opinion. This feature requires the remote doctor to coordinate and participate at the exam, being a constraint to receive in real-time all the information he would have if he was performing the exam locally.
Tele-ultrasonography real-time applications present specific characteristics that demand more network and processing resources from the base computer system. Real-time in this paper means both sides communicating collaboratively and not feeling uncomfortable with the delay. According to Bartoli (2007), this time should be less than 400ms in IP videoconferences to meet ITU (International Telecommunication Union) standards. When the local doctor lacks the knowledge or experience at the medical discipline or the ultrasound interpretation, the remote doctor must take the responsibility for the final exam report. To take this responsibility, the remote doctor must have all the resources and information referred to the exam execution, as if he were in the examination room. For ultrasonography exams, the video of the ultrasound (US) probe position on the patient and a good quality video of the ultrasound exam itself are imperative for such a diagnosis. This way, the communication between both doctors must occur synchronously and in real-time. To obtain the desired quality, several factors related to the network and multimedia areas must be taken into consideration, such as the bandwidth, the audio and video encoding, the processing capability of the involved equipments, and the communication delay. These factors are the key for a good user experience.
The initial motivation to deploy the telemedicine system specifically at the underserved Restinga district (~100,000 inhabitants), in Porto Alegre (~1.5 million inhabitants), was twofold. First, this community needed immediate assistance, as the missing rate in ultrasonography exams was about 60%. Travel from Restinga to downtown Porto Alegre, where ultrasound exams are available is time-consuming (taking nearly an entire day) and expensive for pregnant women, who often have no access to care for their other children while they go for an exam. Second, there was a high bandwidth PLC (Power Line Communication) network installed by the government on that neighborhood.
The development team and the medical team defined the following system requirements:
- Good ultrasound video quality, to show an ultrasonograph’s details (perceptible movements as the heartbeats and the respiratory system). This demand is subjective, and the adequate quality is determined by the doctor when he can distinguish the important parts of the fetus needed to perform the correct examination and taking responsibility for it.
- Audio communication between the specialist doctor and the local resident physician.
- A remote pointer, so that the doctor can pont details to the patient and the local physician (who is with the patient). The remote doctor uses a mouse to position a pointer inside the ultrasound area, and the mouse movements are send to the local place, showing specific areas which the doctor wants more attention.
- A second video showing the hand position of the local physician, focusing mainly in the transducer position on the patient’s abdomen.
- A third video of the remote specialist doctor, allowing the patient to see who is talking with her and the local physician.
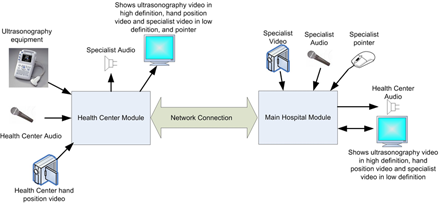
Figure 1 shows a schematic of the developed solution. At the Health Center, there is a non-specialist physician who performs the exam at the patient. At the Main Hospital, it is located the specialist doctor responsible for the report. At both ends, there is audio coding and transmission. In the health center, the system captures the video signal from the ultrasound and the hand position of the attendant, composing both videos on the same screen. The hand position is encoded in low resolution video. Both signals are encoded and transmitted live, being received by the doctor, who analyses it and communicates by video, audio, and through the remote pointer, giving instructions to the attendant and also speaking with the patient.

Figure 1: Overview of the developed solution
![]()
The ultrasound equipment allows freezing selected images and storing in DICOM (Digital Imaging and Communications in Medicine) format for future analysis. The equipment also allows making calibrations with the ultrasound and measuring determined areas, as the fetus’ head diameter and femoral bone size. This is important for the doctor to get the fetus size, comparing to standards and finding growing anomalies.
